What is concussion?
1.1 Introduction
In recent years, there has been increased recognition that American football players are at a higher than normal risk of suffering concussion. Like many other sports, we need to ensure that everyone who participates knows:
1. what concussion is and how serious it can be
2. how to tell when they or a teammate might have suffered a concussion
3. what to do when that happens
4. how long it will take to recover and return to play
This document attempts to address those points. It is based on guidance issued by other sports. It has been developed in conjunction with advice from BAFA’s Medical Review Panel consisting of doctors and other healthcare professionals experienced in the sport and care of its participants.
1.2 Definition
A concussion is a traumatic brain injury that results in a disturbance to the normal working of the brain. In American football, it is most commonly caused by a blow to the head, or by the head forcefully hitting the ground, or a whiplash type effect when the head is shaken by a blow to another part of the body. Concussions most commonly occur without loss of consciousness. Typically, there are subtle indications that a concussion has occurred, such as the player shaking their head, stumbling, or appearing dazed or stunned. The symptoms of concussion typically appear immediately, but sometimes they are delayed and can appear at any time after the initial injury. Playing sport is recognised as one of the main causes of concussion.
1.3 Is concussion serious?
Concussion must be taken seriously, however its effects are not often serious.
The information given here is intended for educational purposes only and is not meant to be a substitute for appropriate medical advice or care. If you believe that you or someone under your care has sustained a concussion, we strongly recommend that you contact a qualified health care professional for appropriate diagnosis and treatment. The authors have made responsible efforts to include accurate and timely information. However, they make no representations or warranties regarding the accuracy of the information contained and specifically disclaim any liability in connection with the content.
Most people who sustain a concussion do not require any treatment, as they normally get better by themselves and recover quickly, without long-term effects. “While the medical term ‘traumatic brain injury’ can sound serious, the actual extent of damage to the brain is usually minimal and does not usually cause long-term problems or complications.” – NHS Choices
While for most the symptoms usually last for a few days, they may last for a few weeks or in a small number of cases longer; when it may be called Post-concussion Syndrome. Research suggests that most adults recover fully by about 7-10 days after the initial injury. During this recovery time however, the brain does appear to be more vulnerable and if another concussion is sustained during this time, the risk of more severe and prolonged symptoms is increased, especially in young players.
This is why it is so important to recognise concussion, remove the player immediately from play, and not allow them to return to play until their brain function has returned to normal and they have been medically cleared.
There is however evidence that repeated episodes of concussion could cause longterm problems with mental abilities and trigger dementia. This type of dementia is known as chronic traumatic encephalopathy (CTE). If you have watched the film Concussion (starring Will Smith) about how the risk to NFL players was discovered, you will understand the potential long-term effects.
There is evidence that players with a history of only two concussions within a year are at greater risk of further brain injury and slower recovery. It is therefore especially important that anyone who suffers repeated concussion should seek specialist medical help. If managed correctly, concussion rarely has serious consequences, and full recovery can be expected.
Most doctors would therefore argue that the physical benefits of taking part in contact sports outweigh the potential risks associated with concussion.
1.4. Is concussion different in young or female players?
Concussions can happen at any age. However, children and adolescents: • are more susceptible to concussion • take longer to recover • have more significant memory and mental processing issues • are more susceptible to rare and dangerous neurological complications, including death caused by a single or second impact.
This is because children’s brains are still developing, and there is concern that concussion can have more of an impact on brain function. There is also evidence that women suffer higher concussion rates than men.
2 How do you prevent concussion?
Concussion cannot be totally prevented, but the risks of it can be reduced. Part of this is by the choice and correct use of helmets, and part of it is by appropriate coaching and playing.
2.1 Helmets
The type and condition of a player’s helmet is thought to affect the risk of sustaining a concussion, due to the transmission of forces to the head and brain. Researchers at Virginia Tech University provide helmet ratings that show different levels of impact 3 protection.
More information on their work can be found at http://www.beam.vt.edu/helmet/.
Helmets with more stars provide a reduction in concussion risk compared to helmets with fewer stars.
2.2 Playing by the rules
Rules Committees have placed increased emphasis on concussion prevention in recent years. Relevant rules include:
• A player must not use the crown of the helmet to make forcible contact against an opponent. As well as a concussion risk, this can also pose a high risk of spinal injury to the player inflicting the blow.
• A player must not make forcible contact against an opponent’s head or neck in many situations where the opponent is “defenceless” and unable to avoid or reduce the impact of any blow. Both of the above are fouls that result in immediate disqualification of the offending player.
It is also a foul for a player to continue playing if their helmet comes off. It must not be replaced while the ball is live – the player must go to the sideline to replace it properly. Coaches have the utmost responsibility to ensure that players block and tackle opponents safely.
The correct techniques need to be taught and practiced until they can be executed reliably. (See also section 6.2 below.)
3 How do you recognise concussion?
Note that in this and subsequent sections, where we use the term “player” it also applies to any other participant in the game who might be at risk of concussion. This includes officials, coaches and sideline staff who might be hit or knocked down on or near the field. We should also emphasis that this document applies to flag football as well as contact football. Head injuries are not unknown at that level.
3.1 Suspecting concussion
Everyone involved in the game, including players, coaches, officials and sideline staff, should be aware of the signs and symptoms of concussion. Clear indicators of concussion include when a player:
• appears dazed or stunned; has a blank or glassy-eyed stare
• appears confused or incoherent
• cannot remember things that happened
• seems slow to answer questions or follow directions, or is easily distracted
• shakes head; grabs or clutches head
• stumbles; has to be physically supported by teammates
• moves clumsily or awkwardly
• shows behaviour or personality changes (e.g. becomes more emotional or irritable)
Other signs include:
• seizure or fit
• loss of consciousness
• disoriented; not aware of where they are
• lying motionless on the ground or very slow to get up off the ground
• blood or clear fluid leaking from the nose or ears
A player might have suffered a concussion if he/she complains of:
•headache
• dizziness
• feeling dazed
• loss or blurring of vision, double vision, or seeing stars or flashing lights
• ringing in the ears or sudden deafness
• sleepiness or fatigue
• stomach ache or pain, nausea or vomiting
• poor coordination
• slurred speech
• poor concentration
3.2 Immediate action on suspicion of concussion
If concussion is suspected on the field, the attention of the officials should be drawn to the player in question. The game will be stopped while the player is removed from the field.
Anyone who recognises the signs should raise an alert with medical personnel (at a game) or a first aider (at training, for example). The player’s coach should also be informed.
The decision should not be left to the player, as they are usually not thinking correctly. Sometimes the symptoms do not become apparent for some time, so in the days following an injury, concussion should be suspected in someone who:
• suffers a drop in work, training or academic performance
• has difficulties with problem solving
• has poor attention or concentration
• has unusual drowsiness or sleep disturbance
• has inappropriate emotions or unusual irritability
• is more nervous or anxious than usual
They should seek medical advice.
3.3 Confirming concussion
Anyone can use the Pocket Concussion Recognition Tool to check symptoms and signs. This can be downloaded from http://bjsm.bmj.com/content/47/5/267.full.pdf.
Healthcare practitioners should use the SCAT3 (or Paediatric SCAT3) to monitor recovery. This can be downloaded from http://bjsm.bmj.com/content/47/5/259.full.pdf.
4 How do you manage concussion when it happens?
4.1Immediate removal from play If you suspect concussion, YOU must REMOVE the player from play immediately.
Continuing to play increases their risk of more severe, and/or longer lasting concussion symptoms, as well as increases their risk of other injury. In young players in particular, it puts them at risk of a fatal brain injury.
4.2 Assessment
A concussion assessment must then be carried out by a professional healthcare practitioner. If one is available at the venue, their assessment must be sought. If one is not available, a first aider must look after the player until an assessment can be made. A first aider cannot clear a player to return to the game – only a professional healthcare practitioner can.
A player removed with suspected or confirmed concussion:
• must not return to play (or any other physical activity) that day
• should not be left alone • should not drive or ride a bike/motorbike
• should not drink alcohol
• needs to rest their body (so avoid running, cycling, swimming, etc.)
• needs to rest their brain (so no reading, television, video games, homework, etc.)
4.3 Flowchart
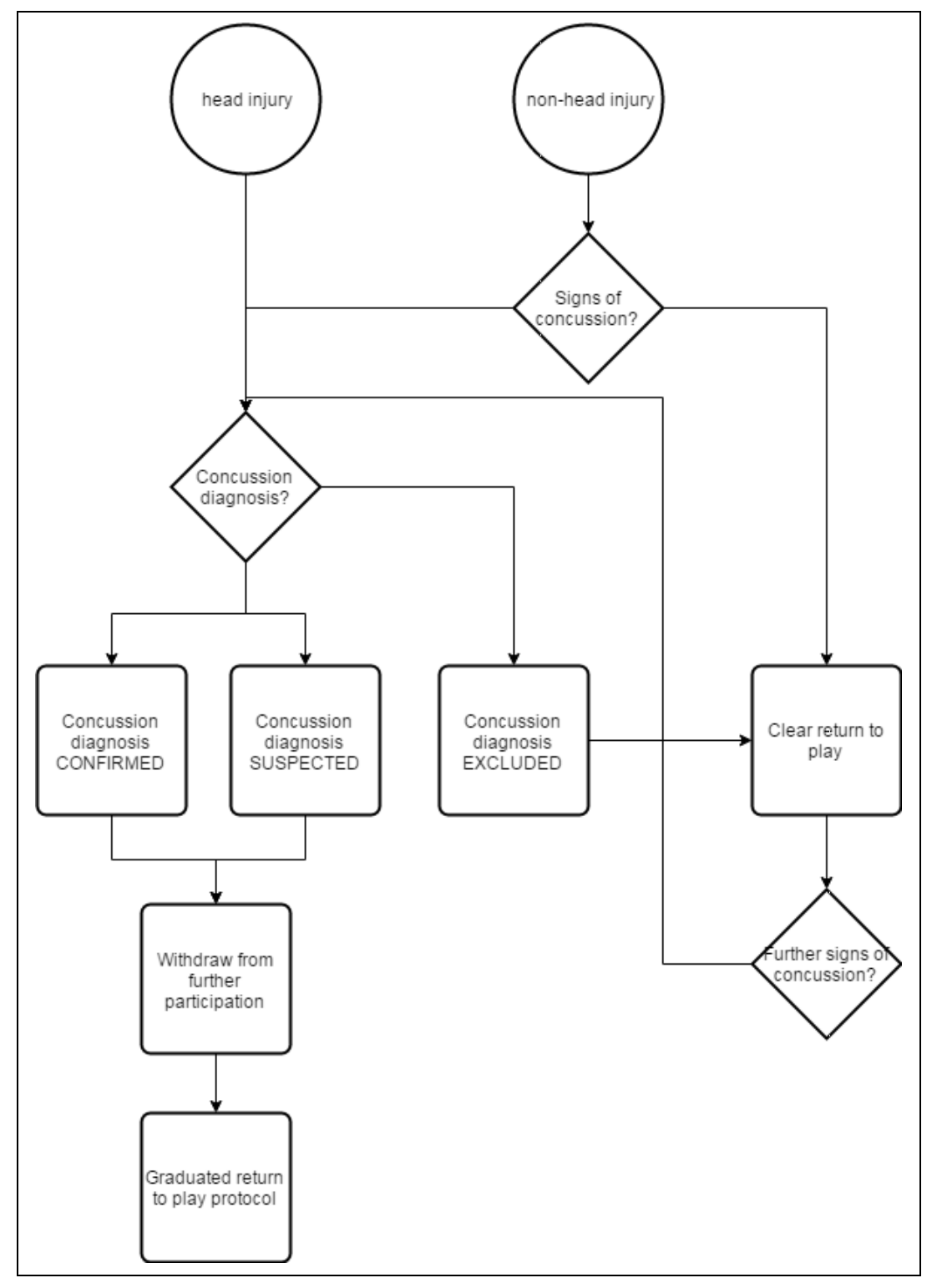
4.4 More serious injury
If any of the following are reported, then the player should be transported for urgent hospital attention:
• severe neck pain
• deteriorating consciousness
• increasing confusion, agitation or irritability
• severe or increasing headache
• repeated vomiting
• unusual behaviour change
• seizure (fit)
• double vision
• weakness or tingling/burning in arms or legs
• difficulty walking
Dial 999 for an ambulance if in doubt about the seriousness of any of these.
4.5 Excluding concussion
The participant may return to play if a professional practitioner has cleared them of a concussion diagnosis, and is confident in that assessment. This decision must be communicated to the referee by the professional practitioner. If in doubt, keep them out.
5 When can players return to play?
5.1General principles
After a concussion, the brain needs to rest, so this means a complete break from physical and brain activities. Sleep is good for recovery, but a balance has to be achieved because too much complete rest is thought to delay recovery.
A return to normal light activities of daily living is advised as soon as symptoms have reduced. No more than 24 hours complete rest is needed in most cases. However, they should not return to sport or physical activity, or any other activity that risks further head injury, for some time. This is normally at least two weeks (see below).
The prohibitions above about being left alone, consuming alcohol or driving apply until all symptoms have gone.
A player may need a day or two off work/study to rest. An employer or education provider may need to be informed of the existence of the injury and reasonable adjustments made to the player’s normal work/study pattern (e.g. assigned desk duties or excused PE).
At all times, if symptoms return, the player must reduce the level of activity, rest and if necessary seek further medical advice. However, despite being symptom-free, the brain is still recovering and remains vulnerable for a period of time.
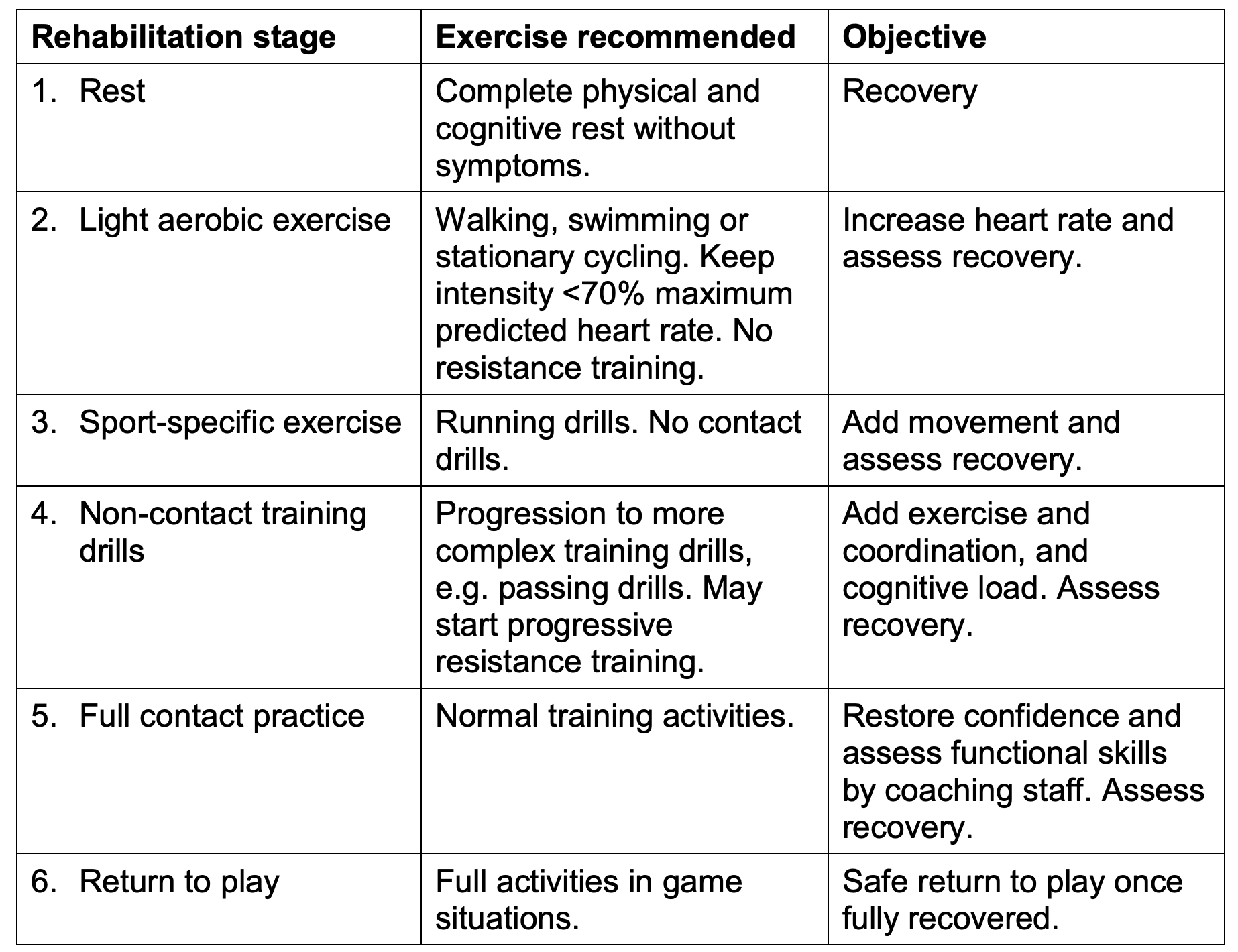
5.2 Graduated return to play
(GRTP) BAFA (in common with many other sports governing bodies) mandates the following return to play protocol.
NB:
Only begins return-to-play protocol after athlete is symptom free
Coaches monitor for a return of symptoms during every stage
Only one stage per day
Move to next stage if athlete remains symptom free for 24 hours following trial
If symptoms reappear, sit the athlete out and return to qualified medical professional
Players must have returned to work/study before starting physical activity (stage 2).
It is recommended that a medical practitioner confirms recovery before entering stage 5 (full contact practice).
Some GPs are happy to clear a player to return to play, but formally clearing players to return to sport is not their role. It is however considered by most experts in concussion that good routine clinical management should include a review by the GP at an appropriate time to confirm recovery and satisfy themselves that there are no other underlying conditions.
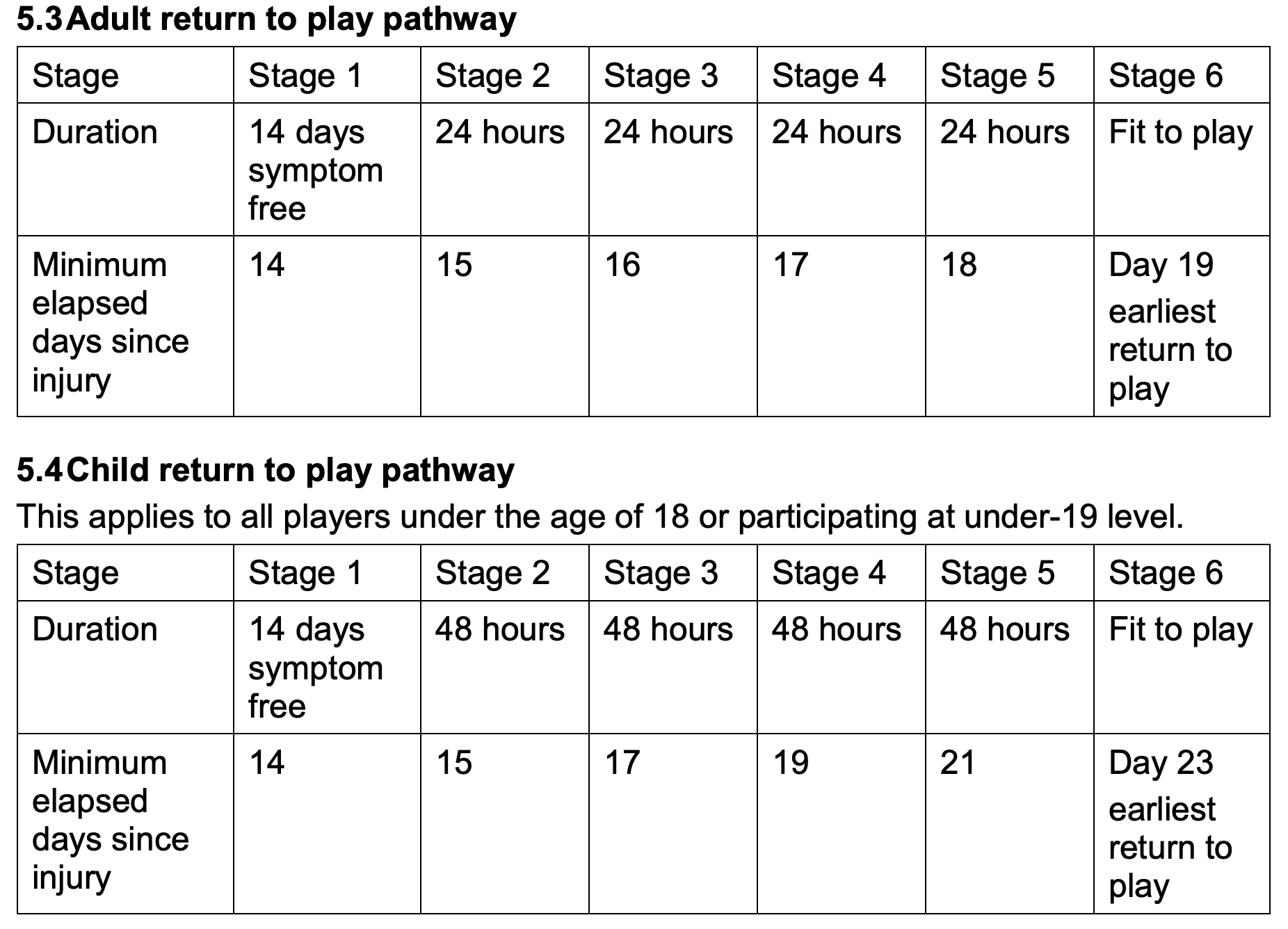
An appropriate time is considered to be around the average time for expected full recovery and before returning to activities with a recognisable risk of head impacts. This fits nicely with the GRTP at around 18 days for adults and 21 days for children. The GP does not need to provide a letter, as verbal confirmation by the player or parent/guardian for U18s is acceptable.
Clubs and schools are advised to make a record of this verbal confirmation. GPs may charge a fee for providing a letter. If it is not feasible for a coach to supervise stages 2-4, these may be done by the player in their own time, or by children supervised by parents with appropriate guidance.
Alternatively, the protocol may be extended with each stage being completed at successive training sessions. If any symptoms recur while going through the stages, an adult player must rest for 24 hours (without symptoms) and then return to the previous stage.
The rest period should be 48 hours for players under 19.
5.5 Responsibilities
The responsibility for managing a graduated return to play is shared by the player, their coaches and their club’s management. Depending on the circumstances, BAFA may take disciplinary action against anyone who is party to a breach of this protocol without specialist medical advice.
Players must remember their duty to inform their coach of their condition and any recurrence of it. Teammates should be alerted to watch out for signs. It is a player’s responsibility (or their parents if they are a child) to obtain medical review before returning to play.
Coaches must be particularly aware of the stage of a player’s recovery and not ask them to do too much. They must always be alert for returning signs of a concussion and cease the player’s activity immediately if they are observed.
Where a player has received specific individual advice or restrictions from a medical practitioner, these should be reported to their club and coach, and must be adhered to at all times until lifted. Even after a graduated return to play has been completed, the player and their coaches must remain vigilant for any return of symptoms.
6 What should coaches and club officers do now?
6.1 Awareness
Clubs should ensure that all personnel are aware of the signs of concussion, the actions to take if concussion is suspected and the graduated return to play protocol if concussion is not cleared. This should be covered at least once per season at a team meeting or training activity.
Personnel who miss that meeting/activity should be made aware by other means. There are a number of resources available to support the education of personnel.
Those provided by England Rugby (http://www.englandrugby.com/concussion) and the Football Association (http://www.thefa.com/get-involved/coach/concussion) are recommended.
BAFRA should ensure that all officials are familiar with this policy, the signs of concussion and the procedures to be followed if concussion is suspected (Rule 13-1- 3 and Appendix C of the rulebook). Officials have a key role to play in identifying players on the field who may have suffered a concussion.
Officials should be encouraged to complete the England Rugby Concussion Awareness training course for match officials (http://www.englandrugbyfiles.com/concussion/courses/matchofficials/).
6.2 Training
Clubs must ensure that they have adequate first aid cover available for all practice sessions where contact will take place. Club personnel, including coaches, should be encouraged to complete first aid courses appropriate to their role. The more first aid trained people available the better. If no first aider is available, practice with contact must not take place.
6.3 Planning
Clubs should plan what they will do if one of their players suffers a concussion.
Who will look after them on the sideline?
Who will take them home?
Who will check up on them during the graduated return to play period, especially the two-week rest from physical activity?
Who will keep an eye on them when they return to practice and ultimately play?
6.4 Coach education
A number of resources are available to support coaches increase their knowledge and awareness of concussion, including:
• BAFCA have endorsed the “Heads Up Football” (HUF) programme promoted by USA Football.
• HUF is a key part of the BAFCA Level 1 coaching qualification.
• BAFCA has run a number of HUF-specific sessions, both at its national convention and at subsequent regional clinics.
Concussion may result from a player’s poor blocking or tackling technique. If this is the case, their coach is responsible for seeing that this is corrected before a player returns to play. If there are concerns about the player’s behaviour and approach to the game when playing or training, that appears to put them at increased risk of concussion or of causing concussion in an opponent, then this should be addressed before return to play.
Players who take an irresponsible approach to concussion perhaps should be asked to sit down until their approach changes. Coaches and club medical personnel need to consider whether to undertake regular CPD to keep their knowledge up to date. At some point in the future, it may become mandatory for coaches to be trained in this.
7 Future work
7.1 Injury surveillance
A major part of improving the safety profile for the sport of American football in Britain is continuing to monitor the rate of injuries sustained during participation. Previously this has been accomplished by evaluating data that has been compiled by those liaising with the sport’s insurers. However, the less than comprehensive nature of this data has raised questions regarding its validity in assessing injury risk.
Therefore, in order to improve our understanding for the benefit of the sport and its participants, we will gradually be bringing in higher levels of injury reporting. Mandatory recording of concussions would constitute part of a nationwide injury surveillance system and a specific injury-reporting tool should be completed to aid these efforts.
7.2 Safety of the game
BAFA continually examines areas within the game where risk for injuries may inform decisions regarding rule changes to eliminate the injury-prone actions or events. We also recognise that sportsmanship plays a crucial role in maintaining player safety, avoiding unnecessary or defenceless contact and collisions, in order to maximise safety and minimise injury risk for all.